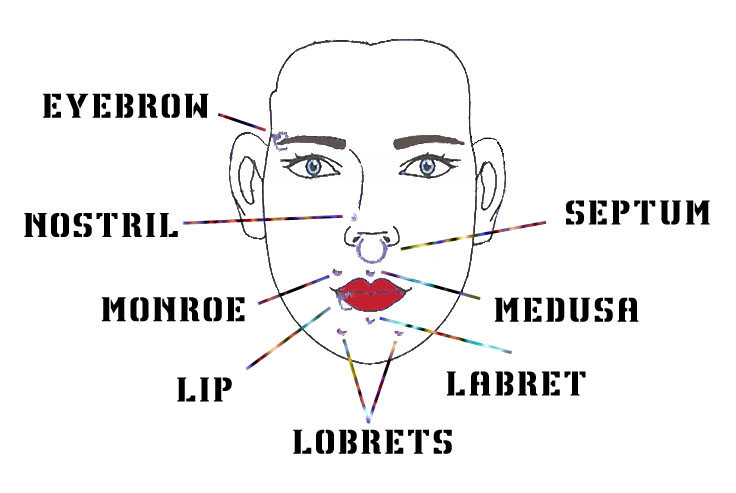
Body piercing indicates the puncturing of a part of the body in which jewelry may be worn. In the last years, oral piercing has particularly spread especially among young people.
Body piercing has to be considered as a surgical procedure to all intents and purposes and, as such, has to be performed only by qualified personnel.
The aim of the present work is to verify which risks patients are concretely exposed to and which complications may occur after an healthcare professional performs oral piercing.
MATERIALS AND METODS
The present study includes one hundred and eight patients (74 males and 34 females) aged between 14 and 39 years, who presented with oral piercing done 12±4 months earlier. After initial counseling, patient medical history was analyzed to identify useful information that could reveal the onset of intraoperative and postoperative complications. Finally, the patients underwent clinical examination to reveal the possible presence of late complications.
RESULTS
After piercing, neither of the 108 patients developed widespread complications. Although all patients said they had followed the piercer’s indications, 96% of them reported postoperative local complications such as bleeding within 12 hours of piercing (90%), perilesional edema for 3±2 days after piercing surgery (80%), persistent mucosal atrophy (70%), enamel abrasions (30%), enamel fractures (30%), gingival recession (25%), erythematous palatal mucosa (15%), dentine hypersensitivity (15%).
DISCUSSION AND CONCLUSION
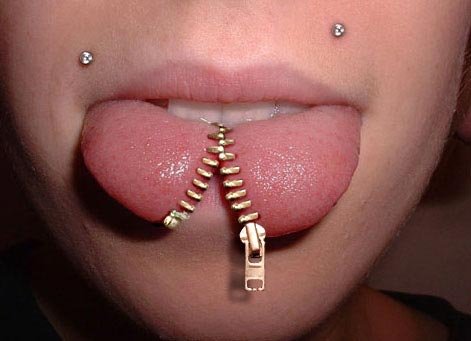
The analysis of results shows that the area that most of the recruited patients prefer to pierce is the tongue: this seems to be in agreement with the recent literature. In fact, It is important to underline that this area is at highest risk for hemorrhagic complications, because of the extensive vascularization in the tongue.
In our study, no systemic complications were identified. However, it seems very important to underline that body piercing should always be done by medical staff in a clean room. As a matter of fact, it is clear that the risk of systemic complications is significantly higher when body piercing is done by untrained personnel without sanitary inspections.
|
|
|
|
|
|
|
|


Congresso Nazionale dei Docenti di Discipline Odontostomatologiche e Chirurgia Maxillo Facciale
Firenze – Siena, 14-16 Aprile 2011
Università degli Studi di Bari Dipartimento di Odontostomatologia e Chirurgia
Direttore: Prof.ssa D. DE VITO
Calabrodental S.r.l. Unità Operativa di Chirurgia Maxillo-Facciale Regione Calabria – Crotone Dir. San: Dott. M. W. Marrelli
AUTHORS
INCHINGOLO F.; INCHINGOLO A.D.; DIPALMA G.; PALLADINO A.; DE CAROLIS M.; TATULLO M.; CAGIANO R.; INCHINGOLO A.M.; PICCIARIELLO V.; MARRELLI M.; ANGELINI V.
REFERENCES
2. N Escudero-Castaño, M.A Perea-García, J Campo-Trapero, Cano-Sánchez, and A Bascones-Martínez. Oral and Perioral Piercing Complications. Open Dent J. 2008; 2: 133–136.
3. Ziebolz D, Stuehmer C, van Nüss K, Hornecker E, Mausberg RF. Complications of tongue piercing: a review of the literature and three case reports. J Contemp Dent Pract. 2009 Nov 1;10(6):E065-71.
4. Kapferer I, Berger K, Stuerz K, Beier US. Self-reported complications with lip and tongue piercing. Quintessence Int. 2010;41:731-737.
5. Hickey BM, Schoch EA, Bigeard L, Musset AM. Complications following oral piercing. A study among 201 young adults in Strasbourg, France. Community Dent Health. 2010 Mar;27(1):35-40.
6. Pires IL, Cota LO, Oliveira AC, Costa JE, Costa FO. Association between periodontal condition and use of tongue piercing: a case-control study. J Clin Periodontol. 2010 Aug 1;37(8):712-8. Epub 2010 Jun 17.