Platelet concentrates for surgical use are innovative tools of regenerative medicine, and were widely tested in oral and maxillofacial surgery. Unfortunately, the literature on the topic is contradictory and the published data are difficult to sort and interpret. In bone graft, implant and reconstructive surgery, the literature is particularly dense about the use of the various forms of Platelet-Rich Plasma (PRP) – Pure Platelet-Rich Plasma (P-PRP) or Leukocyte- and Platelet-Rich Plasma (L-PRP) – but still limited about Platelet-Rich Fibrin (PRF) subfamilies.
In this second article, we describe and discuss the current published knowledge about the use of PRP and PRF during implant placement (particularly as surface treatment for the stimulation of osseointegration), the treatment of peri-implant bone defects (after peri-implantitis, during implantation in an insufficient bone volume or during immediate post-extraction or post-avulsion implantation), the sinuslift procedures and various complex implant-supported treatments.
Other potential applications of the platelet concentrates are also highlighted in maxillofacial reconstructive surgery, for the treatment of patients using bisphosphonates, anticoagulants or with post-tumoral irradiated maxilla.
Finally, we particularly insist on the perspectives in this field, through the description and illustration of the use of L-PRF (Leukocyte- and Platelet-Rich Fibrin) clots and membranes during the regeneration of peri-implant bone defects, during the sinus-lift procedure and during complex implant-supported rehabilitations. The use of L-PRF allowed to define a new therapeutic concept called the Natural Bone Regeneration (NBR) for the reconstruction of the alveolar ridges at the gingival and bone levels.
As it is illustrated in this article, the NBR principles allow to push away some technical limits of global implant-supported rehabilitations, particularly when combined with other powerful biotechnological tools: metronidazole solution, adequate bone substitutes and improved implant designs and surfaces (for example here AstraTech Osseospeed or Intra-Lock Ossean implants).
As a general conclusion, we are currently living a transition period in the use of PRP and PRF in oral and maxillofacial surgery.
PRPs failed to prove strong strategic advantages that could justify their use in daily practice, and the use of most PRP techniques will probably be limited to some very specific applications where satisfactory results have been reached.
Only a few simple, inexpensive and efficient techniques such as the L-PRF will continue to develop in oral and maxillofacial surgery in the next years. This natural evolution illustrates that clinical sciences need concrete and practical solutions, and not hypothetical benefits. The history of platelet concentrates in oral and maxillofacial surgery finally demonstrates also how the techniques evolve and sometimes promote the definition of new therapeutical concepts and clinical protocols in the today’s era of regenerative medicine.
|
|
|
 |
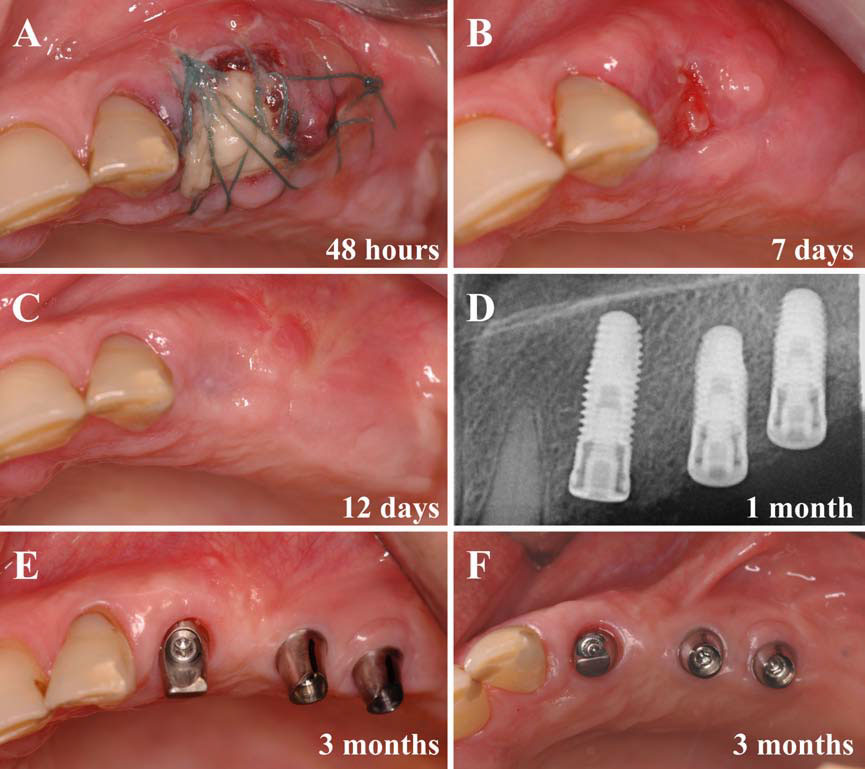 |
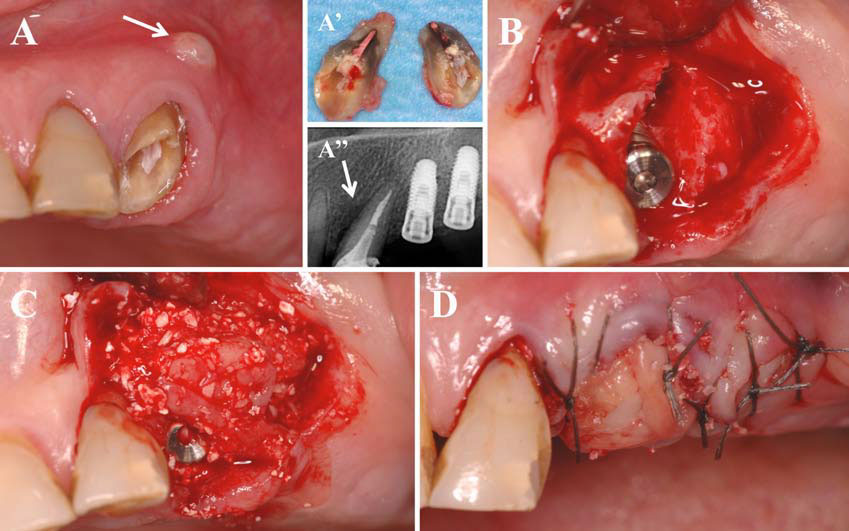
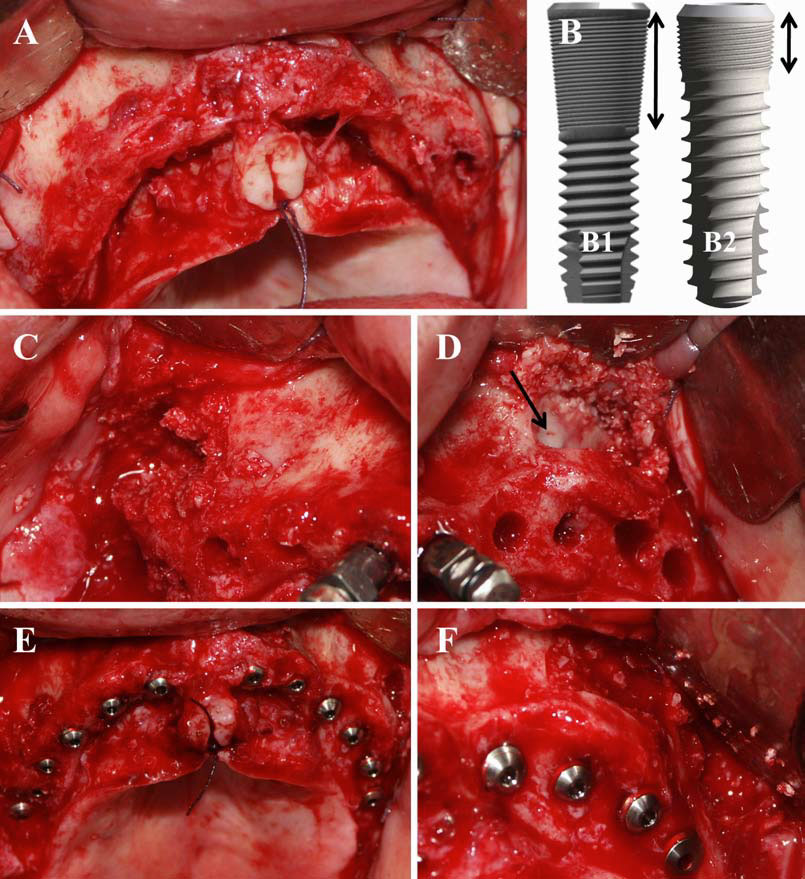
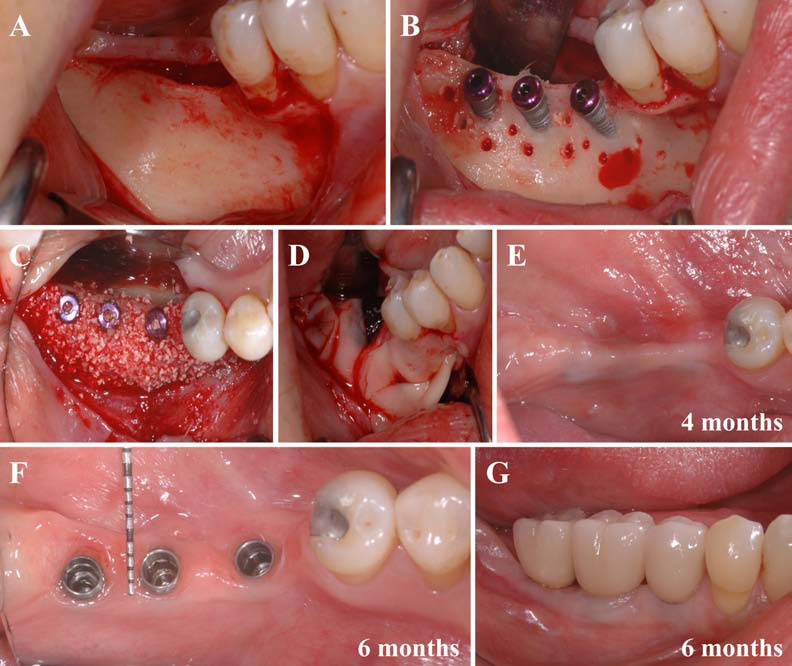
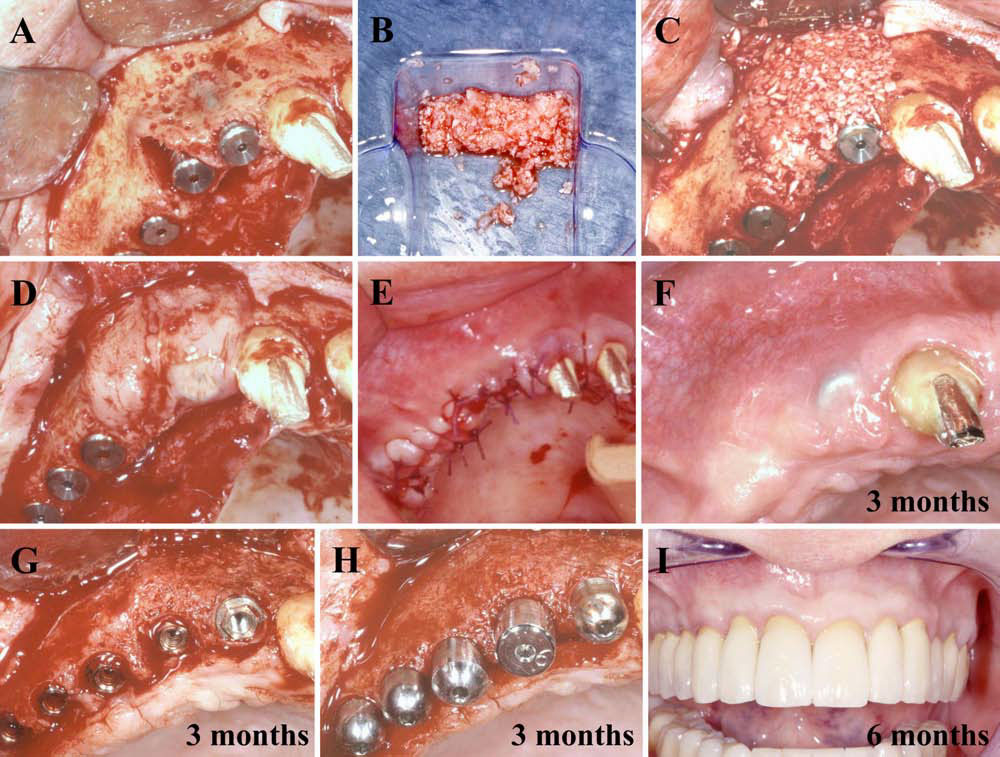
| Fig. (1). Natural Bone Regeneration (NBR) with xenograft of peri-implant bone defects created during implant placement in a thin resorbed alveolar ridge. A. The mandibular posterior alveolar ridge was very thin, and the bone volume was not sufficient for a correct implant placement. B. After implantation, the vestibular faces of the 3 implants (Ossean, Intra-Lock, Boca-Raton, Florida) remained uncovered, resulting in a lower bone anchorage and a serious risk of tissue dehiscences around the implants on a short-term basis. The implants were only blocked by the tip in the bone. The first step of the NBR procedure was to perforate the vestibular cortical bone more than 10 times with a small drill, in order to promote local bone bleeding (endosseous stimulation). C. The vestibular face of the alveolar ridge was then grafted with a mix of L-PRF and xenogeneic collagenated bone (Gen-Os, OsteoBiol, Tecnoss, Italy) in a 50/50 volumic ratio, in association with a 0.5% metronidazole solution. The uncovered threads of the implants were covered, and a significant grafting volume was added in order to regenerate a broad alveolar ridge around the implants. D. Following the NBR principles, several L-PRF layers were added on the grafted area in order to protect the bone material and to stimulate periosteum and soft tissue healing and remodelling. E. Four months after surgery, the keratinized gingival tissue above the implants seemed thick and strong, and the transgingival healing screws could be connected. F and G. Six months after surgery, the healing screws were removed and the final prosthetic restoration was built. The regenerated alveolar ridge was finally quite broad and the gingival tissues were thick and healthy, without dehiscence around the implants. Both bone and soft tissues compartments were regenerated simultaneously by the NBR procedure: this is the synchronized regeneration principle. | Fig. (2). Natural Bone Regeneration (NBR) with allograft of peri-implant bone defects created during immediate post-avulsion implantation. A. In this 65 years old patient treated in 2003, maxillary right lateral incisor and canine were damaged and infected. These teeth were therefore avulsed, the alveolar socket was carefully curetted and drilled for immediate post-avulsion implantation. The implants were blocked in the residual bone, but there were a large bone defect around the canine implant and a vestibular fenestration in front of the lateral incisor implant. The first step of the NBR procedure was to perforate the vestibular cortical bone with a small drill, in order to promote local bone bleeding (endosseous stimulation). Note that 3 other implants were also placed in the posterior right edentulous ridge. B. A bone grafting material was prepared using a mix of L-PRF and freeze-dried bone allograft (Phoenix allograft, TBF, Mions, France) in a 50/50 volumic ratio, in association with a 0.5% metronidazole solution. C. The grafting material was used to fill the peri-implant defects and also to cover and thicken the fenestrated vestibular bone ridge. The canine convex contour was recreated with the material. D. L-PRF membranes were covering the grafted area, stabilizing the grafting material and protecting the bone regeneration compartment. E. Tight sutures were performed. The gingival flap had to be pulled up the implanted and grafted alveolar sockets, since the covering tissue after the avulsions was too short. F. Three months after surgery, the gingival tissue was healed and thick, particularly above the former avulsion sockets. However, one cover screw was observable through ; the gingival tissue was quite thin in this area, probably because the implant head was too prominent after implantation, leading to mechanical constraints on the healing gingiva. G and H. Three months after implantation, the cover screws were removed and the transgingival healing screws could be connected. We observed that the peri-implant bone defects were completely regenerated and the vestibular side of the alveolar ridge was thickened. The grafted volume could not be distinguished from the original alveolar bone. I. Six months after implantation, the final prosthetic rehabilitation was performed. The final result was both very esthetic and functional, particularly in this complex case where bone volumes and soft tissues were compromised. Seven years after the treatment, the clinical result is still stable with no notable evolution of the bone levels or gingival aspect. | Fig. (3). Natural Bone Regeneration (NBR) with xenograft around peri-implant bone defects during immediate post-avulsion implantation in an infected avulsion socket. A, A’ and A’’. The left maxillary canine root was infected and associated with a large vestibular fistula (A, white arrow). The root was in fact broken, as observed after avulsion (A’). A deep periodontal lesion was observed on the radiograph (A’’, white arrow), the periodontal bone was infected and compromised. B. The root was carefully avulsed, the avulsion socket was curetted and drilled for implant placement. The implant was blocked in the residual bone walls, but the peri-implant defect remained largely opened. C. The periimplant defect was filled with a mix of L-PRF and xenogeneic collagenated bone (Gen-Os, OsteoBiol, Tecnoss, Italy) in a 50/50 volumic ratio, in association with a 0.5% metronidazole solution. The destroyed bone anatomy was restored with the bone grafting material. D. The grafted area was covered with a triple L-PRF layer in order to stabilize and protect the grafting volume from the oral environment. The gingival flap was damaged and too short after the avulsion for the complete covering of the implantation site, and tight sutures were not possible. The implantation site was therefore only covered and protected by the L-PRF layers, kept in direct contact with the oral environment. | Fig. (4). Natural Bone Regeneration (NBR) with xenograft around peri-implant bone defects during immediate post-avulsion implantation in an infected avulsion socket. A. 48 hours after implantation, the strong superficial L-PRF membranes were still present and protecting the grafted area. The gingival tissue was in the induction phase and highly proliferative. B. Seven days after implantation, the gingival tissue was still proliferative, but the hole above the avulsion socket was filled with a reddish neo-tissue: the L-PRF matrix had supported the surface reepithelialization and merged with the gingival flap into a regenerated connective tissue. C. Twelve days only after implantation, the surgical site was completely closed and already thick and strong. We were still in the remodelling phase. D. The radiographic follow-up after 1 month revealed an homogeneous bone quality around the implant, and no sign of the initial infection and defect. E and F. Two months after implantation, the transgingival healing screws were placed. One month later, the prosthetic abutments were connected to the implants. Three months after implantation, the alveolar ridge was perfectly healed and presented a large bone contour and a thick and stable peri-implant gingival tissue. |
 |
 |
 |
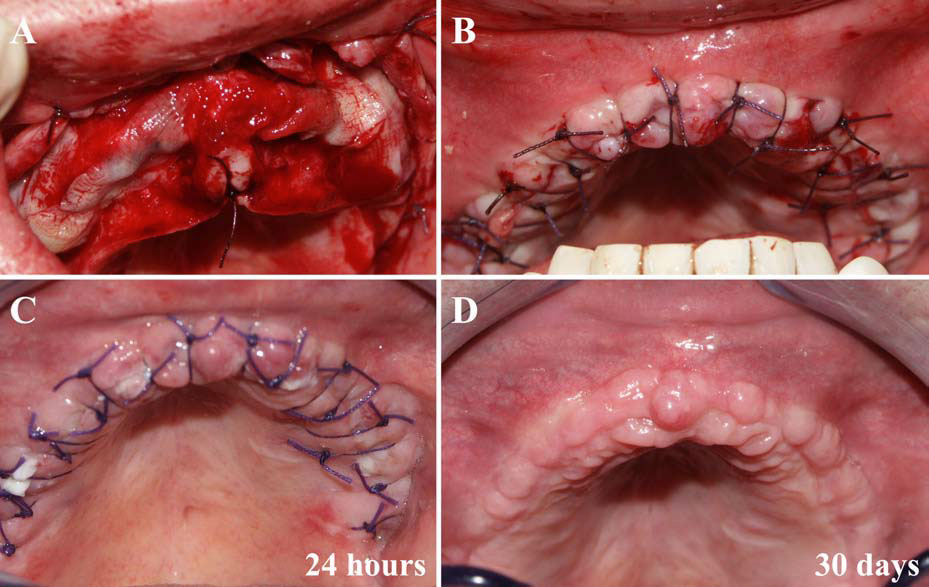 |
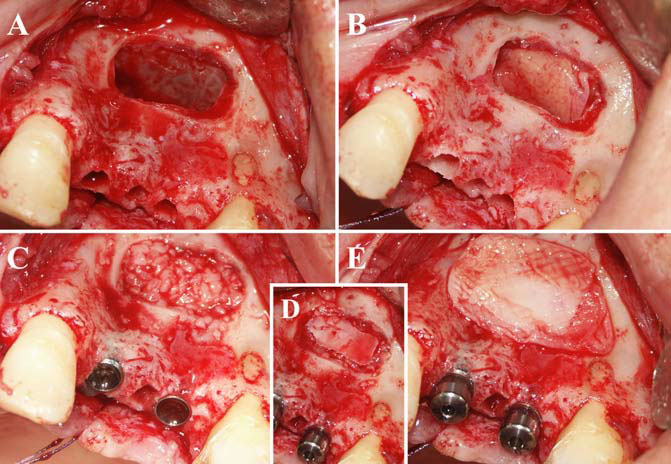
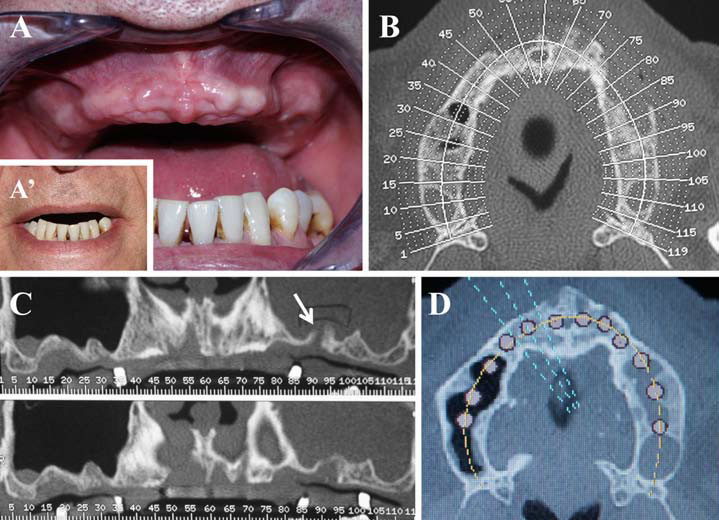
| Fig. (5). Natural Bone Regeneration (NBR) during a sinus-lift procedure with simultaneous implant placement and L-PRF as sole filling material. A. After the lateral osteotomy, the Schneiderian membrane was lifted and therefore protected when the implant drillings were done. B. Two L-PRF membranes were placed to cover the Schneiderian membrane. C. Two Ossean Intra-Lock implants (Boca-Raton, Florida) were inserted and the implant tips were in contact with the L-PRF layer in order to maintain the Schneiderian membrane in high position. The subsinus cavity was then filled with L-PRF clots. D and E. The osteotomy window was closed with the original osteotomy bone fragment, and finally covered with a last L-PRF layer before sutures. | Fig. (6). Global implant-supported rehabilitation of the damaged maxillary using L-PRF, with bilateral sinus-lift and simultaneous implant placement. Initial situation. A and A’. This 57 years old patient presented a severe centripetal alveolar resorption with irregular alveolar ridges and gingival tissues, associated with the loss of the upper lip support. B and C. The X-ray tomodensitometric examination highlighted the major resorptions of the alveolar ridges, an uneven residual bone contour with many large bone defects (particularly on the left side), and a millimeter-thick subsinus residual bone height (SA4 sinus). In addition, the left sinus was filled with a large inflammatory mucous thickening, without clinical signs, seemingly caused by the infectious alveolar site around the left residual maxillary molar (white arrow). After avulsion a few months before, the tooth left behind a crater which resulted in a small oral-sinus communication. D. A surgical planification software was used on the X-ray scanner radiograph. The ideal positioning of the dental implants required to regenerate bone in the sinus and in several alveolar bone defects. This computed study was important for the validation of the therapeutic strategy in this resorbed and damaged maxilla. Using the L-PRF and the NBR principles, it was decided to achieve the complete implantation of the maxilla, with double sinus-lift and simultaneous implant placement in SA4 sinus. | Fig. (7). Global implant-supported rehabilitation of the damaged maxillary using L-PRF, with bilateral sinus-lift and simultaneous implant placement. Surgical phase. A. The surgical site was largely opened, revealing the uneven bone contour and the perforation of the left posterior alveolar ridge (the oral-sinus communication). B. In complex rehabilitations, the use of improved implant design and surfaces is recommended, such as Osseospeed (B1, AstraTech, Mölndal, Sweden) or Ossean (B2, Intra-Lock, Boca-Raton, Florida, USA). These implants present a microthreaded collar (black arrows) that allows to block the implant in a millimeter-thick residual bone height and is therefore particularly useful in the subsinus area. C and D. After lateral osteotomy, the sinus membranes were lifted on both sides. The implant drilling was performed in the residual bone height, and the Schneiderian membranes were finally covered with a L-PRF layer (black arrow). The alveolar ridges were also corrected in order to keep a more regular contour. On the left side, the damaged alveolar area was curetted and finally the small oral-sinus communication was drilled in order to block an implant inside. E and F. The subsinus cavities were filled with a mix of LPRF and freeze-dried bone allograft (Phoenix allograft, TBF, Mions, France) in a 50/50 volumic ratio, in association with a 0.5% metronidazole solution. Twelve AstraTech Osseospeed implants were then inserted and blocked in the residual alveolar ridges. On the left side, an implant was blocked successfully in the former oral-sinus communication. The same bone grafting combined material was used to fill the numerous bone defects of the alveolar ridges around the implants. | Fig. (8). Global implant-supported rehabilitation of the damaged maxillary using L-PRF, with bilateral sinus-lift and simultaneous implant placement. Early healing. A. The alveolar ridges were covered with L-PRF layers in order to protect the grafted material below and to improve the gingival healing and remodelling. B. The flaps were pulled up and tight sutures were performed in order to protect the grafted compartment, leading to a risk of insufficient vestibular keratinized gingiva. C. 24 hours after surgery, the incision line was almost closed, because of the healing stimulation promoted by the L-PRF layers. We were in the induction phase of the L-PRF-stimulated healing, and the gingiva seemed very proliferative. Post-operative pain and edema were also limited, as it was always reported when L-PRF layers are used to promote early neoangiogenesis on a wounded site. D. Thirty days after the surgery, gingival healing was complete and we were in the remodelling phase. However, the gingival surface was still uneven and proliferative. The thickening of the keratinized gingiva had been induced by the L-PRF layer and lasted several months. |
 |
 |
||
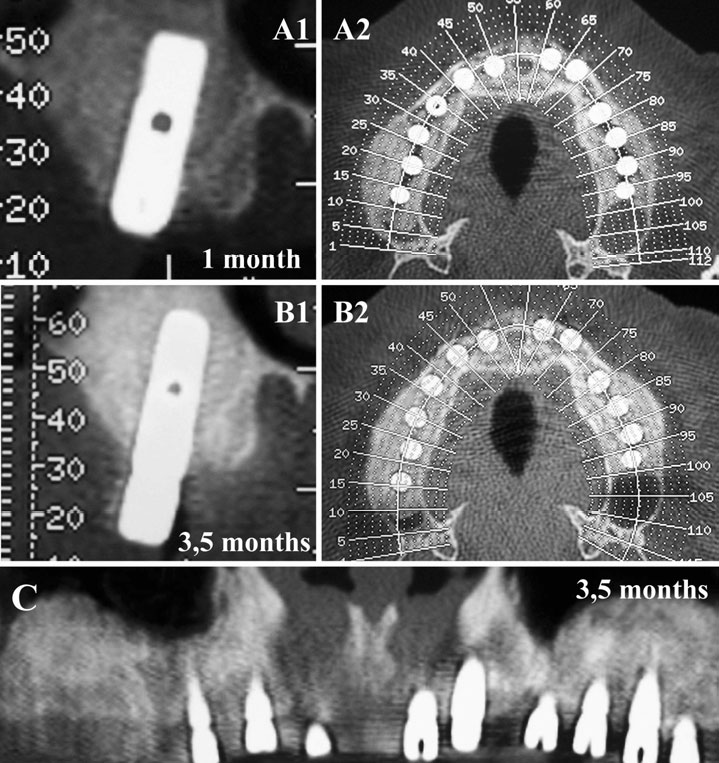
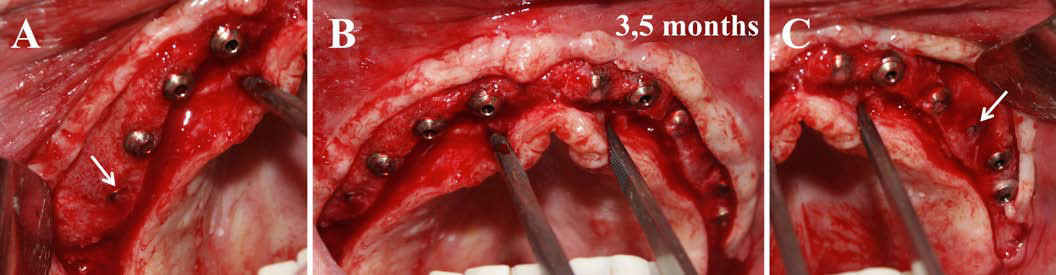
| Fig. (9). Global implant-supported rehabilitation of the damaged maxillary using L-PRF, with bilateral sinus-lift and simultaneous implant placement. Radiographic follow-up. A1 and A2. One month after surgery, a first X-ray tomodensitometric examination was performed. The large grafted area seemed homogeneous and stable (because of the metronidazole protection), but not very dense. B1, B2 and C. The scanner taken 3.5 months post-operatively showed the high homogeneity and density of the grafted volume, particularly in the sinus-lift area. Moreover, the large intra-sinus mucous proliferative inflammation had completely disappeared, probably because of a synergy of factors (antiinfectious effect of metronidazole, and the stimulation of healing, neoangiogeneis and the associated drainage promoted by the L-PRF). The comparison of radiological bone densities on the scanners taken at 1 month and 3.5 months post-operatively illustrated the evolution of the density of the grafted volumes. The quality of the bone after 3.5 months suggested that the implants were ready for function and final prosthetic restoration. | Fig. (10). Global implant-supported rehabilitation of the damaged maxillary using L-PRF, with bilateral sinus-lift and simultaneous implant placement. Reopening. Three and a half months (105 days) after implantation, the surgical site was reopened in order to remove the cover screws and to connect the transgingival healing screws. The grafted bone tissue displayed a dense and homogenous aspect and could not be distinguished from the original alveolar ridge. The L-PRF layers stimulated the periosteum and some implant heads were covered by new regenerated bone (white arrows) that had to be eliminated. The gingival flap was thick and homogeneous. | ||
 |
|||
| Fig. (11). Global implant-supported rehabilitation of the damaged maxillary using L-PRF, with bilateral sinus-lift and simultaneous implant placement. Final healing. A. In order to promote a repetitive induction on the gingival tissues, L-PRF layers were placed around the transgingival healing screws, and the gingival flaps were then sutured around the implant heads. B. 6 weeks after the second surgical phase, the gingival tissue was completely healed and very thick, but still displayed a proliferative aspect because of the second L-PRF induction. It was then possible to start the prosthetic phase. C. The healing screws were then removed for the preparation of the final implant-supported prosthesis. The thickness and quality of the peri-implant keratinized gingiva were considerable, and were the keys for a long-term esthetic and functional result. Finally, despite the initial significant maxillary bone resorption, the treatment lasted only less than 6 months. Five years after the treatment, the peri-implant bone levels and soft tissues are very stable. This successful strategy was driven by the use of L-PRF and associated biotechnologies. | |||
AUTHORS
Alain Simonpieri, Marco Del Corso, Alain Vervelle1, Ryo Jimbo, Francesco Inchingolo, Gilberto Sammartino and David M. Dohan Ehrenfest
THIS IS ONLY ABSTRACT. THE FULL ARTICLE IS AVAILABLE DOWN